Atlas Musculature: Dysfunctions III,1,2
| MYONET - Atlas Musculature Orofacial System |
Atlas Musculature: Dysfunctions III,1,2 |
Erhard Thiele 024e |
| Atlas Musculature Inventory | MYONET.TOTAL PROGR CONTENTS |
Discourse about the Muscular Faulty Functions of the Muscles of Area III
– Diaphragma Oris and Velum Palatinum –
Oral diaphragm hypertension forces the tongue body up and forward straight into the oral cavity or even more forward ( what is to be found frequently with extroverted persons but as well in syndromes like the DOWN) und, thus, may simulate a too big tongue. Without the mouth floor musculature powerful tongue movements are not easily imaginable, hyperfunction of the tongue rather not possible. Assuming a missing diaphragm tonicity (hypofunction) then, necessarily, those muscles linking the tongue to its vicinity - the extrinsic - would have to substitute the abutment function what, fore once, would be incomplete, else would lead to overstraining. In another connection we discussed that emergency programs installed from the organism to grant the claimed functional results of an action in case of an impairment of some sub-organ would overload the not concerned system components, overstrain them and in the long run damage them. In case of an activity deficit of the oral diaphragm musculature the whole deglutition action would be aggravated; the result would be swallowing through gravity (as we observe it on patients having difficulties taking "pills"). One speciality should also be mentioned here. It is the low pressure which exists in the oral cavity in rest position and function with the mouth closed. It is created through sinking the oral diaphragm, rostrally sealed with the lip closure and retrally through the Velum palatinum and the multiple upper pharynx musculature, as already described. In some cases stress might create a too strong low pressure which through a widespread centripetal force would have an unfavourable effect on the hard substance capsule ("ball-shell-model"). There would be only one thinkable case when a strong low pressure would be physiological, when in the case of the physiological oral self-cleaning the interdental spaces would be sucked clean. Else this state will have damaging effects. Diagnosable this state gets through the consequences on the soft tissue surfaces as, for example, the horizontal buccogingival ridge in the level of the occlusion plane of the dental arches on the Vestibulum mucosa (see picture 18071080110-01 to 03, below). As with the before discussed soft tissue impressions also in this case a respective disorder will result in tooth marks on the inside of lips and cheeks. As the air pressure mechanism only works when the mouth floor is shut towards the pharynx in this connection in short terms the anatomy of the Velum palatinum should be discussed. The velum consists of a tendinous-muscular flap being covered with mucosa on both sides; it holds a multiple mobility. The median part of the lower ridge contains the Uvula with an own musculature. To muscles serve for the sail adjusting, the Tensor and the Levator. For the respective purpose and particular functions the oral respectively nasal cavity can separately be tightly closed through the flap (see discussion about low pressure) for nose breathing, eating, drinking and critical sound formation ( cue: Rhinophobia). In the caudal direction the flap muscualture continues into two palatine arches pulling the velum down to near it to the tongue base. To be mentioned: M. palatohyoideus und M. palatoglossus.
Over the last years a special field of therapy gained significance, the neuromuscular respiratory tract disorders like choking, snoring and sleep-apnoea. As with all sensomotor dysregulations it is as well in these cases difficult to determine whether the accent in those defects lies more on the muscular or the neural side. The therapeutic approaches are multiple and include the medicamentous treatment, for example with sedatives, over the mechanical technique like the respiratory mask, the combination of both, mask and oxygen up to manipulation via a dental splint. To all these methods a therapeutic chance can be admitted less it may be seen in a rather mental effect. Closer investigations should define whether texture changes have lead to the reported symptoms. In such cases the described methods are rather insufficient as a surgical correction seems advisable. If the cases belong to neural or mental respectively regulation problems - which as is well known are resulting in muscular transformations - as well alternative therapy methods should be advanced; in our case the training of sensomotor complaints through neuromuscular exercises from Myofunctional Therapy as they are described in: "Theorie und Praxis der MFT Bd 3, Myofunktionelle Therapie, Katalog der Übungen zur neuromotorischen Funktionsregulation in chapter „Mundrückraumübungen“,S.87 [The special part of this website MYONET in the section: "Myofunctional Therapy Catalogue of Exercises for a Neuromuscular Function Regulation", chapter BACK-OF-MOUTH-EXERCISES]
 |
 |
 |
|
 |
|
||
| Abb. 18071080110-01 to 05, disturbed inside/outside balance. On the left upper picture the area on the inside of the lower lip is marked with a white circle where the surface is squeezed between the upper and lower canines to form a transversal fold of 2 to 3 cm. The indentations at the rim show the imprint of the teeth. | |||
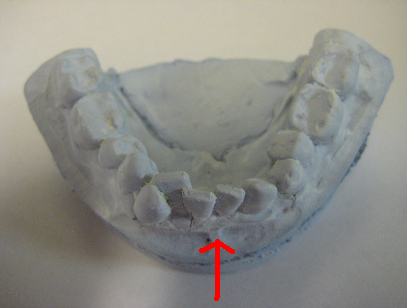
| The two lower pictures show models of jaws, left the interocclusal state demonstrating the inclination angle of the upper incisors rim the outward tilting while the lower front is pushed back and the dental arch collapsed, the latter more impressively visualised on the right picture seen from above. | |||
After having described the musculature of the tongue, oral diaphragm and palate next the extremely important therapeutic field including the deglutition act will be described citing the Rauber-Kopsch.