Atlas Musculature: Physiology,I
| MYONET - Atlas Musculature Orofacial System |
Atlas Musculature: Physiology,I |
Erhard Thiele 010e |
| Atlas Musculature Inventory | MYONET.TOTAL PROGR CONTENTS |
1.1.2 Discussion of the Physiology of the Muscles of Area I
– Orofacial System –
The orofacial musculature will have to be discussed in this connection presumably under the viewpoints being of interest under the viewpoints of Myofunctional Therapy. For this purpose the listed literature has been taken to counsel.
J. W. Rohen writes in his functional Anatomy: (re-translated from the German Language)
”All muscles are striocellular and strongly interwoven so that their bundles preparatively hardly separable. The lower and lateral fibre groups are linked with the Platysma. All fibre groups together are forming a functional System which grants a multiplex play of movement around the oral aperture. The complicated construction of the mimic musculature in the mouth region can not be explained solely from the functional necessity of the masticatory system. Here beyond the mechanical functions a highly differentiated locomotor system has developed which gains an additional significance for speech and expressive movement of the face. [136, S. 241].
Do we make observations about the function, we are used to see the musculature as the dynamic element moving the osseous skeleton and so being under its command. Yet already from the evolution musculature is primary and dominant.
The osseous skeleton has been formed in the succession of development and thus helped musculature to an improvement of its function. It is coined by musculature, gets shaped by musculature and is subjected by musculature to a continuous adaptation and transformation.
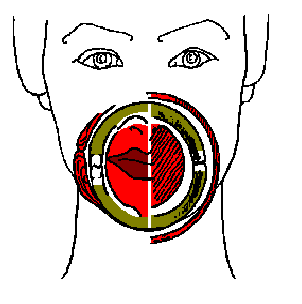
Seeing the relationship musculature / skeleton under this perspective (bones are the crutches of musculature) we will realise that - functionally as well - that the osseous structures are imbedded in a dynamic equilibrium of synergists and antagonists of the musculature. Applying this to the face it means that the face in its family resemblance is not moulded out of some plasticine in a similar way and then filled with life. But rather: The programming of the muscle actions (movement pattern) and its tonicity are inherited and thus will lead through the coining of the osseous armature to that unique family resemblance. As figurative comparisons may serve the comprehension we will imagine the orofacial system with facial skull and musculature as a brittle hard shell, Lets see this as an antique bulb-like vase having been restored from its shreds. In its interior it is kept from collapsing by a rubber ball, at its exterior coated by a rubber cover. This forms a layering of spheres stacked one inside the other (like the Russian "matryoshka" dolls). This "ball-cup" assembly, thus, contained in its core a rubber ball which were sustaining an outward directed pressure - centrifugal - the outside cover, though, pressing centripetally. The tension of inside balloon and outside mantle being in equilibrium in its pressure, the bulb-shell in between, the "vase" stays in a stabile form. Our "Balloon" inside is represented by the tongue musculature, supported by the oral diaphragm, the "cover" outside is formed by the orofacial musculature. The "vase" is the osseous upper and lower jawbone with its alveolar processes and dental arches. This picture will serve us well with understanding the physiology and its pathological alterations. Here in the discussion of the physiology we will now and firstly turn to the "cover", the orofacial musculature. During the embryonic development our "rubber cover" is very easily to be recognised. In image 19 and 20 a picture (Rauber-Kopsch) from the 7th week of human embryonic development has been projected on our model (19) whereas image 20 shows the mimic musculature of a grown-up (quote Rohen[136,page241].
|
|
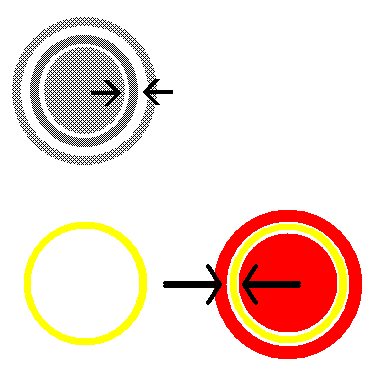
Abb. 16: Bulb-Shell Model |
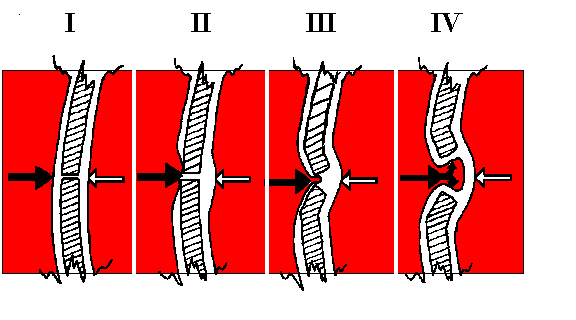
Schematic drawing representing the inside-outside equilibrium of forces in the oral system. Disorders may appear as well through air pressure differences as from muscular incongruencies between inside and out. In this connection see also the pictures on Page 24. Mostly a combination of both causes will be present. The sequence mechanism of the deformation in such a disorder is shown in picture (16a) below. Primarily the skilled eyes will merely note a muscular deficit, later on followed by a bending-out; soft tissue portions are urging in between and, thus, accelerating the process See also model photo page 24.
|
|
|