Atlas Musculature: Physiology VII
| MYONET - Atlas Musculature Orofacial System |
Atlas Musculature: Physiology VII |
Erhard Thiele 033e |
| Atlas Musculature Inventory | MYONET.TOTAL PROGR CONTENTS |
| VII/4. (M. pterygoideus lateralis) |
|
The Lateralis is formed of an upper and a lower part both of which comply with different tasks in operating the joints at different phases of the mastication process. The lower part initiates the opening movement. Both parts are functioning simultaneously in the protrusion, unilaterally (lateroprotrusive, collaterally) when grinding. The upper part directs the joint during the closure which brings us to the special construction of the joints. The temporomandibular joints (TMJ) are constantly acting in pairs but in different ways depending on the required movement, whether solely symmetrically in respect to the median line or for the opening in combination with a sideways shifting, or in lateroprotrusion. Even a slight backshift is possible. This requires a special joint construction. The TMJ conducts a gliding/rotating motion. In a simplified description it shows a socket with an attached ramp and, facing the joint head, a cartilaginous 'washer' functioning as a sled. (It would be a somewhat simplistic simile to envisage a winter sportsman -the joint head - gliding down a snow slope on a plastic bowl with a grasp; we would have to imagine the whole thing reflected upside down; the gravitation in tobogganing would be comparable to the muscle power for the TM joint pulling in the direction of the socket. The advantage in this comparison would be: The sleigher, in the unfavourable case, might after a bum come to sit in front or behind the sled and harm the seat of the pants, like the joint head!) Let us leave the disorders of this field to the gnathologists. They frequently deal with patients being deranged around the stomatognathic system, here mostly with late cases, adults or relapses. In those cases via the orofacial system the whole stomatognathic and craniocervical (superordinate) system drawn into the symptomatology. A predominant reason for the fact that we rarely find as well symptoms of the disease in the stomatognathic system may be seen in the fact that the development of the joints will be completed not until the end of the tooth change. In adult TMJ-patients we find an interesting kind of tongue dysfunction - a substitute or protective function of the tongue: When the teeth in the side region are missing partially or completely the tongue gets laid between the alveolar arches of the jaw bones to fill the gap. After replacing the teeth (in some technical way) at first when chewing the edges of the tongue are getting in between the teeth. Grinders quite frequently insert the tongue between the masticatory plains as a sort of bite splint as protection - s bad shield! Joint disorders generated by dysfunctions are to be seen in our special field if the position of the Mandibula is involved as, for example, with frontal or lateral tongue biting on or nibbling at respectively foreign bodies and items. Joint disorders are further arising after the tooth position has been changed through orofacial dysfunctions secondarily drawing the joints into the disease. All joint movements especially the mouth opening are if not also operated through the ventral and antagonistically dorsal neck musculature (supra and sub hyoidal and neck musculature - see later - ) so rather al least necessarily compensated for stabilisation through the dorsal and ventral muscles. We should mind that the TMJ is a pendulous joint and this also for our functional muscle exercises. It served this function already when we still were walking 'on all fours'. The dental arches pressed upon each other are unfavourable for the joints especially with a simultaneous shifting of the mandible in the sagittal direction (protrusive or retrusive). These positions should never be asked for in the muscle training exercises. It is completely unnecessary to list up more correlations between orofacial disorders and stomatognathic symptoms. You could well say that every unsolved orofacial case will end up in a stomatognathic late case - most frequently through a shifting of the tooth position (jaw bone loss).
Function movements of the mandible and their muscular background To summarize the responsibilities of the hyoid muscles for the mandible movement already discussed in the respective chapters the following table is cited from Rauber-Kopsch [126, S. 744] |
|
Lowering of the mandible (Abduction): |
Lifting of the mandible (Adduction): |
Grinding movement Working side |
Balance side |
|
M. digastricus |
M. temporalis |
M. digastricus |
M. temporalis |
| M. mylohyoideus | M. masseter | M. mylohyoideus |
M. pterygoideus medialis |
| M. geniohyoideus | M. pterygoideus medialis | M. geniohyoideus | M. pterygoideus lateralis (Pars inferior) |
|
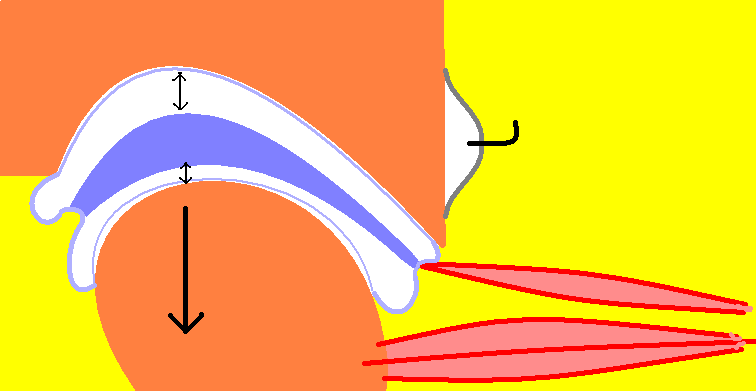
M. pterygoideus lateralis (Pars inferior): initiation of the movement |
M. pterygoideus lateralis (Pars superior):Fixation of the Caput mandibulae at the Tuberculum declivity |
M. temporalis (Pars posterior) and M. pterygoideus lateralis (Pars superior): Stabilisation of the Caput mandibulae |
|
| Muscle exercises: Having followed this link get back to this page with 'arrow back' on your browser ) | ||
| EXERCISE | Working muscle | Action/Effect |
|
OPEN AND CLOSE 049 |
Adductors Temporalis, Masseter | Strain relief, harmonisation, orientation |
|
THE PEA 029 |
Jaw opener and -closer | Orientation, synchronisation, TM joint |
|
JOINT-EXERCISES 201 |
(annotation to the collection of suitable exercises) | Generally therapeutic |
|
JOINT STRETCH (MANIPULATED) 096 |
Adductors , strain relief | Strain relief through manipulation (Physiotherapy) |
|
CHEW AT THE BACK 071 |
All chewing muscles | Coordination, retrusive posture |
|
JAW EXERCISES 205 |
Synopsis of all muscles for the mandible movement | Physiological movement frame |
|
MASSETER EXERCISE 118 |
Adductors | Hypotonic muscles, active training |
|
GAPE 099 |
Joint- and adductor mobility | Tissue stretching |
|
TIRE OUT CHEWING 052 |
Chewing muscles | Steadying by tiring out |
|
,DRAWER-IN’-EXERCISE (CHIN-IN) 028 |
Temporalis rostralis, Pterygoideus medialis | Relaxation by orientation |
|
SIDE THRUST 137 |
Temporalis rostralis, Pterygoideus medialis, unilateral | Relaxation by manipulated stretching |
|
TAP-TAP’-EXERCISE 098 |
Chewing muscles | Tonicity regulation through Sensitation |
|
TONGUE PROP 089 |
Adductors | Jaw occlusion, deflection from adductors to the tongue musculature |
|
As hinted at on the previous page there is a therapy topic which demands
special attention by the Myofunctional Therapy, the medical condition of the
Juvenile Idiopathic Arthritis (JIA). This implies the possibility of an
inflammatory alteration of the joint tissues (socket and capitulum surface)
as well as the Discus Intercondylaris and corresponding ligaments - see
schematic sketch..
|
|
 |
In the also above
mentioned publication on the website of the CCMF has been pointed out in
detail that any splinting will hinder the development of the facial skull
being in the state of development implying that here, according as to the
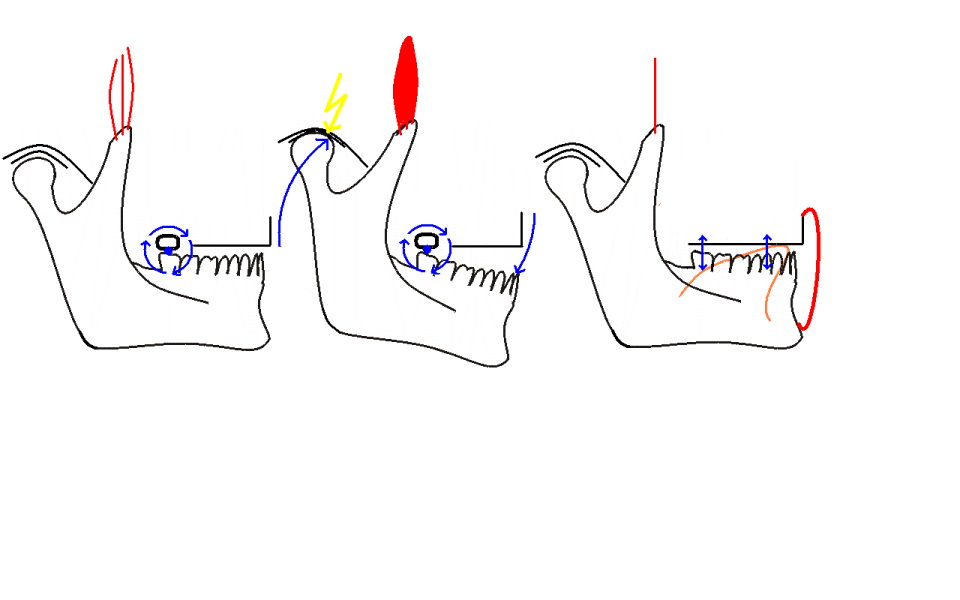
special anatomy, muscle training should have the priority. As the picture on
the left demonstrates it is not sufficient to limit the efforts on the
unloading of the adductors (Masseter, Temporalis). Tensioned adductors cause
a rotating tilt of the Corpus Mandibulae around an imagined axis in the last
molar whereas the Capitulum is shifted to cranial-medial burdening the joint
passways in an atypical manner (left picture 1 and 2). To respond to this
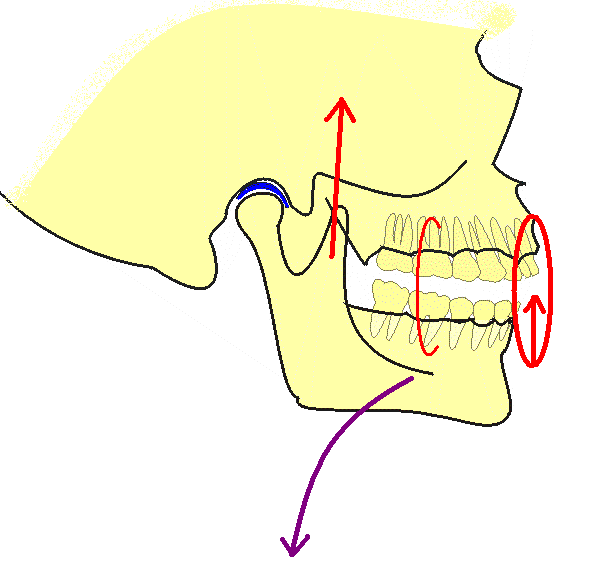
movement the mandibular body has to be evenly suspended and balanced through
a 'net' of muscle tracks (picture 3 on the left and sketch on the right). To
achieve this the extrinsic tongue musculature and the perioral muscles will
have to be integrated.
|
 |
Regarding the special required muscle exercises see the respective chapter.