
General
Chapter
INTRODUCTION
TO THE E-BOOK
Myofunktional Exercise Collection
|
Start |
Contents |
MFT-Start |
to the Catalogue |
MFT-guide |
MFT |
Catalogue |
|
|
General Chapter
|
INTRODUCTION TO THE E-BOOK |
Myofunktional Exercise Collection |
|
A Piece of Advice in Front: |
F |
|
Every This
collection will only be valuable for readers who knows its content. This will be facilitated by the fact that the general structuring for every chapter/exercise got a paragraph at its beginning with the title ,Application’ where the assignment is described. In the table of contents a number of chapters behind the name are showing the notice in brackets (general). It makes sense to read these chapters in front because in these you find pooled a special kind of exercises for a special purpose discussed and listed. You may have noticed that, at the end of each page, a link leads to the subsequent page. And yo may also have found on the left side of the page ‘catalogstart’ a register of the page sequence. So you can always return to this page in order to link up to a position of your choice, maybe directly to the page ‘exercise list’where you may call on the exercise desired. |
|
|
Systematics in Myofunctional Therapy |
|
|
|
|
Let us assume we would in fact plan our treatment procedure.
Then there are several topics to be regarded An earlier publication in the Jour´nal of the IAOM (Thiele,E.: Timing In Myofunctional Training, The International Journal Of Orofacial Myology, November 1996, Volume XXII Page 28-31)
also addressed this topic.
Moreover there are certain ways to combine these different
modes and / or different exercises ( described in the chapters about the
TIMING).
|
| I am not going to discuss each
of these topics in detail. My favourite subjects this time are -to reveal the background of a disturbed function, -to compare it to the background of the normal, fit and physiological function, -to spot the defects -to conceive a scheme for readjusting the correct, normal, physiological background pattern. This requires three items of background information present before my inner eye: 1. The genetic key function of the concerned part of the organism 2. The layout of the function background 3. The complete equipment of our methods, mainly exercises. I did not especially mention the fact that I, of course, should precisely know the normal function of the system considered. There surely are many other topics to be regarded. Just think of the detectives work to spot a disorder - spying out the patients habits, secretly watching him during the conversation, looking for "fingerprints of the villain" on the whole body and asking either precise or hidden questions. This is to say that we will frequently be confronted with the “function gains form” variation, when we are looking for those “fingerprints of the villain” named dysfunction. In many people’s heads the clearly dominating structure of the body is what seems most resistant against force or decay. They see the body as one of those coat trees or hallstands that we find in our hotel room, designed to put the cloths on. That would be the skeleton of the body. The soft tissue, pulled over it, completes the figure. |
|
I mentioned the key function of the genetic development. Here
it exhibits its significance. What is the genetic key function of the musculature? Genetic Demand. The Evolution. It is basic for the understanding of the self regulating neuromuscular mechanisms (of our therapy region) to consider, how structure and function of this region have developed. All in all we started from the single cell (see illustration), stuck to a host environment and got bigger, which means, the cells multiplied forming a multicellular conglomerate which, probably through selection, got to hat we are. For the most time we were only soft tissue and for quite some time a muscle tube. What was the reason to go this way? Ingestion, eating! The longer the food stuff stays in direct vicinity to the secreting and absorbing cells of the body surface (outside, respectively inside), the better is the effect. The more protected the effect is going on, the higher the amount of the result. If I clear my remains into the inrushing provisions, the usable stuff will not be that fresh. I consequently open up a second hole in the pouch (representing my body to that date) for the take-in. I will soon learn that, when I squeeze myself together, the whole procedure is accelerated in quite an advancing way. So I come to let pulses of squeeze run along my hose shaped body, soon recognizing, that I not only press the stuff trough my tubular inside but am pressing the whole tube forward, turning up fresh stuff. The peristalsis has helped me with new bits and pieces so far, but no new source was occupied. The wobbly duct does not make me a good walker. At length, when my constant endeavour has resulted in stiffening chondruous oblong alterations within my muscle layer, and when I have decided to make some use of it, the path is free to finally walking ahead. The muscles have created their crutches and they will continue to form and adapt them perpetually. A little rough draft will help to elucidate this developmental Process. Following the green arrow it the developmental process starts with the single cell gets a visitor, couples and starts proliferation – 1 – 2 – 4 – 8 – 16 – passing the Morula-stage then the bubble „Blastula“ followed by the invagination „Gastrula“, stretching and creation of a second opening besides the primal mouth, later on followed by the Amphioxus stage where chondrous stiffeners begin stabilising the body. The basic idea in this development so far seems to be how the cells can be optimally nourished when their conglomerate more and more increases in size. With a small cluster of cells each single cell can serve itself from the ambient solution of the host environment. In a bigger cluster the inwards sited cells do not get their share why the hollow sphere develops. Its cells must take up their nutrients out of the onrushing matrix. The following invagination favours a digestion process as the matrix, now, does no longer rush past and so improves the effect of the ferments and so gains a better absorption of the matter. The deeper the invagination, the more effective the process. Only, as already hinted at, digestion remnants and fresh nutriment is mixed up. The solution for this special problem comes with the hollow tube and its direction of flow through in the worm stage. And from there on it is not far to the peristalsis of the muscle tube which is interesting us so much and which is not only advancing the nutrient through the worm but straightway the worm through the nutrient. With the increasing demands on the choice of the environment in respect of the quality of the foodstuff the mobility has to be improved what leads to a stabilization of the frame, next, through commutation of muscle fibres into chondrous spikes which, later on, get ossified in the direction of vertebrates. So much, by the way, about the predominance of musculature over bone and function gaining form. |
|
In our case of trying to diagnose a muscle function problem
it will less be “function gains form” but rather: “malfunction gains
malformation”. |
|
My first impression of the patient
will come from looking into his face. It has the effect of compressing the dental arches, leading to their collapse. In earlier publication I compared this structure of our skeleton with the procedure of the reconstruction of the fragments of an antique amphora where a specialist reconstructs the pieces to its former shape by gluing them together on a soft support which resembles a blown-up air balloon while the outer pressure is adapted with the aid of a rubber foil. |
|
This example elucidates the influence of the inner and outer facial musculature upon the bone. This reminds to the old saying: "If you do not stop drawing faces it will some day suddenly stay like that". Or: "From a certain age everybody is responsible for his own physiognomy." This leads to the conclusion that for our muscles bone is like wax. If we, now, look for hints to track down neuromuscular problems we should investigate for more evidence rising from our own observations respectively from results of our neighbouring disciplines; Muscle lesions, neural malfunctions (like the Multiple Movement Syndrom) or innate defects. In this connection we should remember that a defect in a neuromuscular system rather tends to aggravate due to the additional and atypical charging of the textures. This originates from the continuous abnormal load put on the system as it is functioning under the steady strain to generate the lifesaving effect it is created for, regardless of its present functioning in an emergency program. This, then, also applies to the excessive demands towards the abilities of the (to date) not affected system parts. These conditions will, in the long term, destroy it slowly but steadily. The system is not able to retain the Physiological frame which, at the end, will collapse. For the troubleshooting we should again use a special scheme: In this connection we might rather not discuss the 'scanning' of the Orofacial Musculature with the aid of the Diagnostic Exercises. These are also available on this website under this link. Just as much as this: We have available the adequate exercise for every kind of Muscle Function Test. After you have worked off every single Muscle Function Test (taking into account every muscle and / or function of this area) you will have got a quite sure picture about localisation and degree of the dysfunction. Diagnostic Exercises as well as Tonometer Exercises (for measuring muscle strength) are to be looked up under the respective shown link. In the mean time the Tonometer has undergone a certain ageing process and, I am afraid, has sadly been overtaken by an electronic device of a friendly related colleague. Although... the Tonometer is quite a robust device even in the hands of children (and underwater - however it should have got there). Be that as it may, I will conduct this as the second step. My first step will always be the search for visible changes on the textures: Face forms, as mentioned, lip line forms, tongue structure, the form of the palate and dental arch and, of course visible functions as sound formation, respiration, mouth posture and all sorts of visible Habits and the referred markings. An unbalanced antagonistic muscle pressure for example as in the mentioned outer and inner muscle system of the oral cavity will result in for the orthodontist so characteristic dislocation of hard textures like bone and teeth as dental tipping; consequences of unbalanced muscle power will lead to a progressive disorganisation thus leading to further deformations. |
|
We mentioned the sphere shell model for the facial skull with its inner muscle bulb and the outer muscle coat which keep the hard textures in between as long balanced in an indifferent position as the muscle power is balanced -similar to the pointer of a scale.
Leaving this matter we come back to arranging a therapy. This is, as shown, an important task for example for the sports trainer: The methodology of arranging muscle exercises to effective training units. How do you see or use the contents of an exercise? dynamic, static, strengthening, relaxing? How do you combine exercises to a session in a way that they gain more efficiency through this specific combination when they boost each other? This resembles physiotherapy, fitness training. What, again, reminds me to that I wanted to write about this new measuring device we mentioned before. There was a discussion at one of the meetings of the CCMF in Germany (To throw that in: We had to cancel our working group for Myofunctional Therapy, the: AK-MFT - Arbeitskreis für Myofunktionelle Therapie - years ago because of administrative reasons. The 'rest' or hard core consented in founding a sort of scientific Web Company, the CCMF - study group 'Cervico Craniale Myo Function ' - visit us in the internet (www.ccmf.de ). But, back to the mentioned physiotherapy or fitness training: You will know these fitness devices in those fitness studios which are helping us to shape our muscles or keeping those old joints moving. My colleague Klaus Berndsen has presented a device which is intended to make therapy shorter and more efficient by using an appliance which has the only purpose to make our Muscle Function Exercises more effective. For further details please look at our website http://www.ccmf.de/ or at his, the: http://www.isst-unna.de keyword 'Faceformer'. When reading about the success he gains with that appliance you might feel compelled to analyze the background how this measure is efficient. There are quite a number of proposals for the use of devices for fighting grinding, snoring, mouth-breathing, not-breathing at night, tongue malpositioning and all those things which make our so muscle function dependent life this difficult and interesting. To give a precise definition of my premises: Effective appliances for our training concept - should support wanted physiological actions, - should move within the physiological frame. Let us take a snoring aid as the example. The device is made of acrylic in the common horse-shoe shape. It resembles the teeth protector of a boxing champ (where it really makes sense - not to mention the fat that it does not really make much sense for me to punch ones jaw). Quite similar implements are known as splints for the stabilisation of teeth especially for people who might loose their teeth through grinding or bruxing. These units might be useful to a certain degree if constructed in the proper manner to adapt to the neuromuscular performance of jaw and joint movements. (See Paper "Die Temporomandibulargelenke im Formenkreis der rheumatischen Erkrankungen" [The Temporomandibular Joints in the Spectrum Disorder of Rheumatic Diseases] zum Symposion an der Rheumaklinik in Garmisch-Partenkirchen im Januar 2011 [at the Symposium of the Rheumatism Clinic Garmisch-Partenkirchen , January 2011). Instead these devices are constructed in a manner to force the jaw forward by positioning the mandibular dental arch frontally to its physiological intercuspidation. After a lengthy application you could notice a backing-off of the jaw bone while the dental arch is caught in the non-intercuspidative rostral position. This results then in a steady shifting of the teeth in their bone bed connected with a lot of difficulties with chewing and followed by damages in the muscles, the joints and, of course, in the periodontium of the teeth. One fact is crucial for all devices invading neuromuscular processes: They should never stop, hinder or suppress anything by force as this will induce nonphysiological reactions, feelings, motions and last not least tissue alterations.
Our systems are well able in a high degree to adapt to environmental requirements within their 'normal' physiological range of functions. The 'normal function' may be defined as : Gaining the desired effect - with optimum result - under minimum stress. At the other had, forced to create the desired effect under nonphysiological conditions, for example to overcome a tissue alteration, working under an exaggerated muscle hypertonicity or under some 'funny device' will lead to further damage within the system and its surroundings. The device will have to be measure of assistance for the system but not measure of constraint. Furthermore - mostly the therapeutic success will not be stable when the device is deposed. If we decide to apply any device we should conscientiously weigh the pros and contras. If you tried to follow my trains of thought: The thing we talked about, the Anti Bruxer Splint (so called night guard) - it may, indeed, help people who are in a chaotic situation when they are about to grind their teeth out, aware of this, but not quite knowing what to do about it. Before we can teach them some suitable method of Myofunctional or Mental Training there has to be immediate help. Now, what will happen the very moment we put the splint into the mouth? Provided that we tried to consider every possible gnathologic/myofunctional aspect with the construction - Positive comments first: There exists a mental access for the whole procedure. The patient positions the splint into his mouth, conscious of it being beneficial for him and stopping him grinding his teeth. That will be of some worth for him. The second aspect is of a solely gnathologic nature. If the splint is constructed correctly it will provide a front-canine-guidance which means that through the sensor cells in the canines (Mechanotransduction) the self-controlling neuromuscular feed-back circuit gets activated. It seemed to me that with the moment of incorporation switches were thrown and the control function started to work. The third positive point might, more or less, be disregarded; it is related to the mere mechanical function of grinding the teeth together. By means of the splint they may stabilizes each other while the attrition is refined to the plastic material.
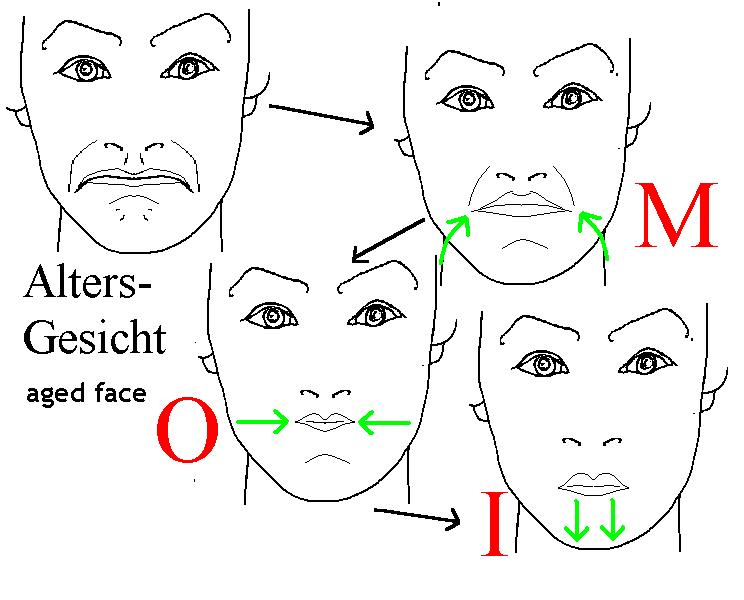
The negative aspect is directed towards the logical, the physiological reaction of the control centre. Some material gets into the mouth - the information is transmitted upwards to the masticatory centre and immediately answered with the order "Chew!" It is precisely this we wanted to stop. Under this viewpoint of myofunction the splint turns out to be contra productive. The second reason for contra productivity is equally seen from our perspective, again: There is no educational or training or educational value in this method. The whole thing is a crutch and only a crutch. Is a crutch a therapy? Now, back to my initial remarks about devices for our therapeutic efforts. They may, indeed, be beneficial if they brave your careful and systematic inquiries for all thinkable effects. In principle - what is helpful for the disorder must not be helpful for everything? Think of the small rubber ringlet, the Elastic. Known and famous as The Myofunctional Therapy! In certain cases it may, indeed, be helpful. That reminds us of some other viewpoint: The Master plan for a physiologically working system is: Gain the desired effect with optimum result under minimum system stress. Each action the system is not designed for will load decided stress on its components with the consequence of damage. If, therefore, we want to gain a sufficient result we cannot turn a blind eye on the fact whether the result has been generated from a physiologically working system or really even through an emergency process given to guarantee health for a short provisional moment within the rules of adaptation. Concerning the 'hardware' an operative system is vital for the textures under a loop (feed-back): Adapting does not mean transmute. If the system adapts from within itself the sequence of the process steps will stay the same. The intensity may be changed just to meet the changed demands. An adaptation to a changed degree of activity should not inevitably bring about changes in the textures. Nevertheless it frequently does - think of the aging athlete or the 'Tennis-arm' - myogelotic alterations within the muscle fibres and inflamed joints through a long-lasting muscle hypertonia. Of course this can also be found in the masticatory system, the tongue muscles, in any part of the orofacial system. Just think about the celebrities with their surgically restored baby-doll faces who try to avoid texture alterations in the form of wrinkle formation by getting the respective skin muscles paralysed with Botox injections. (It would be a rewarding challenge to teach these people rather not to ill-use their musculature - a special chapter (,MOI') of the exercise collection deals with the problem of elderly people's faces). To come back to our problem: Adaptation is by far not so damaging. What really harms is conversion, the transmutation of the textures of a neuromuscular system. Processes like that may be found throughout the organism. This mostly results from injuries. One link in an action chain had been harmed or destroyed. Now the system must arrange the action without this member. The result will in most cases be defective and incompetent while the remaining active respectively overactive chain members will suffer heavy damage by the time. What nature teaches us in this case is that our therapeutic procedure will have to fall into line with the scheme, not decide on it. Here and for now we will be content with the three mentioned items: Genetic key function, functional background, therapeutic armamentarium. The first one, the genomic imprinting has already been discussed. Musculature dominates bone, it has developed, created it. It is a fundamental fact from time immemorial and valid down to the present day. If a malformed bone structure exists we should realise which muscle is functioning respectively dys-functioning in this area. The little story about the evolution more over hints towards another fact. Most muscles we are dealing with in our special field have developed their charcteristics out of the ancient patterns as, for example, the peristalsis movement of the muscle tube, the worm, and mainly from the lifesaving reason of food intake, the digestion and the hunting (physiologic basic condition! Life saving!) Face muscles have differentiated from one single muscle sheath (anatomy). Remember the worm stage with one inner and one outer layer. Even quite highly developed mammal embryos as in humans in early stages show that uniform muscle layer of the face musculature. Having that fact in mind this will inevitably influence anamnesis and diagnosis. This is not confined to the mentioned areas. Considering the genesis of a body part certain processes of vital reactions will, in respect of their genetic presetting, per se be in- respectively excluded. Regarding our examples: Having the peristalsis of the muscle tube from the worm phase in mind the single steps of the swallowing reflex chain will explain themselves. ( Having the Amphioxus stage respectively the developmental step with the branchial arches in mind I will not ask why the trachea entrance is positioned in front oft that from the oesophagus. The gills are below, there, where the (respiration) water is floating through; the filtered-out nutriments pass straight on!)
And quite similar runs the explanation about the development phase for the differentiation of the said muscle sheeth into more or less distinctive muscle tracks in the Orofacial Musculature. This explains why some people simply can not separately move different adjoining tracks because they are just not differentiated into single tracks. Nevertheless we must find an acceptable solution how to provide satisfying neuromuscular actions and results.
Our topic 2.: The layout of the functional background. Our experience with the evolution conveys that are in many cases we are confronted with a ,historical ' self-adjusting mechanism, a feed-back circuit with a short-cut reaction: Control Center - Efferent Pathway - Nerv ending at the muscle (the visibly working part) - Receptor Cell upon it (registrating conditions and announcing it to the center) - Afferent Pathway - Control Center. A quite interesting detail this circuit is running on, a biomechanical principle: It all depends on the Mechanotransduction. If the receptor cell gets unter some kind of mechanical pressure it will transform this into electrical pulses which, then, can be transferred to the control center. Let us imagine this circuit with a frame around it, a "Green Frame". It will be of special interest for us as it stands for the 'Physiological Frame' ('physiological' shall mean lifesaving, as we already have defined) within the borders of which the system functions or at least should function by playing out all its integrated qualities (or 'frame conditions'). We might imagine the whole system as a mosaic picture or jigsaw puzzle where every single part of it stands for one quality of a neuromuscular system - those indispensable 'ingredients' which enable its correct functioning and, thus, the lifesaving effet as this is the destination of a system within the organism: Physiologic = Lifesaving.
The Jigsaw Picture What are these Qualities?
ORIENTATION
SENSITATION
MABILITY
MOTILITY
TONICITY
COODINATION
HABITUATION
They are listed up here in this specific order seen from the viewpoint of the therapist. Let us take an example from Dental Medicine. We today are, as mentioned, more and more occupied by the stress disorder jaw pressing and this in its most diverse forms. If I intend to change anything I will, first of all, have to direct both of us, Patient and therapist, trough the initially mentioned preparatory measures to gain the Compliance' = Understand the necessity for a change;
- notice the deficiency
- have the willingness for a change
- be ready to cooperate.
Quite an interesting topic! It made me write my first book and to draw it, a, as people would today call it "Workbook" with task cards for children. It is commonly called 'Zungenkämpfer', the tongue fighter. The book tries to make the patients feel like a sportsman in a competition. But this is not our talking point here. We want to find the best way for a start. When I tell a patient that he is grinding his teeth from 99% of the cases I will get pitiful glances. They do not notice that. The system by the time has received thousandfold warning signals over the feed-back. In a sort of overflow-reaction the subconscious mind has at last overlooked all signals. Afterwards the system has raised the sensitivity threshold. Functionality now is no longer granted, Sensitivity no longer protects the components. Hypo-Sensitivity. For this reason it is a fundamental task to evaluate feeling and to re-establish it, the Sensitivity. This will be the first step, as well in diagnosis as in therapy. When the system learns, relearns to perceive the proceeding of an action, as well inside as concerning the effect this creates the basis to "arrange the correct size of the mosaic stone for the functioning puzzle picture within its 'Green Frame'.
Then we just go on with the other qualities which either do or do not fit into the frame. In a picturesqu comparison the seven qualities may be seen in a chain; a chain is damaged if only one of its links is broken. What we have got to do is: Test every single link to localise the defekt. For the next link (Quality) in the chain we will enable the patient not only to feel' whether' but also 'where'. In our example with the bruxer: "Is your moth tightly closed or hanging loose?" This step stands for: Orientation, to know in wich position the system is localised. The reader will have noticed that our criteria do not only fit for the orofacial region but indeed for every neuromuscular system in the whole body. For example the intervertebral disc diseases. Try to point out to him that he contiually walks in a wrong posture, sits or sleep triggering asymmetric muscle cramping and, thus, causing a skelettal distortion which compresses the intervertebral discs asymmetrically. Or, for example, the habitually slightly raised position of an arm leading to a very sportive disorder, the Tennis-arm. The delinquent will just not realise the wrong position he not even senses any position! (Only if directing his full attention towards the certain body part.) It will therefore be our next task to mediate a sens to the patient in what position the actual body part is just located, or more precisely expressed, when something is located in the wrong position. As for the arm it would not be too difficult. It is still less challenging with the outer face muscles. This is the reason why we are commonly working withbthe hand mirror. The optical control. With the inner muisculature it becomes more difficult as with the stomatognathic / orofacial which mostly is hidden from the direct view. But as we, indeed, have exercises at hand for nearly every case we might assumethat we do create a possibility to feel the special body part we are working at. So our next task will be to provide him with the possibility to feel the part in relation to the surrounding which means to orientate it. As all previously mentioned qualities of a physiological process (the 'Green Frame') are linked up tightly wit one another we can very well discuss them individually but never treat them individually. They, just as in the puzzle picture, are interlocked with one another. In nature there is no borderline between Sensitivity and Orientation, one depends upon the other quite the same way as our exercises for it. It should be put in here that the order in the succession of the listing of the Qualities is not chosen by chance. Each one does not function without the one preceeding it in the list. You practically can not bring an extremity into a fitting posture without feeling it, and without the Orientation an appropriate Mobility is unthinkable, it obeys the laws of orientation - if it can! And this is the problem our next task starts with. For reasons of definition now the difference between the next two terms shall be explained. Mo-T-ility with the T in the middle differs as we shall see quite plainly from the Mo-B-ility with the B with which we describe the ability of a mneuromuscular system to move - within its physiological borders. Its Move-ability. If it can not keep the borders of its Green Frame, if it functions hyper or hypo this will be a case for us. Possibly the ability to move is restricted ba a tissue blockage or it may, in contrary, be overstretched. Both issues deserve our schooling, primarily to organise the movements within the prescribed borders and, next, to reorganise the tissue components. All that to give the movement the correctform. The next thing would be the correct sequence or flow of the movement which brings us to the already mentioned Mo-T-ility, the performance. If a neuromuscular system is apt to be moved, if it is mobil, this does not per se include that it would actually move, Or as well, the kind of movement, frequent or scarse, powerful or weak; this all mainly depends on the control software (while with mobility it rather depende upon the construction of the hardware). This fact takes us directly to the next Quality in our list. the Tonicity or Tone. Tonicity mainly depends on the muscle tone which in turn is depending upon the tonicity of the neural systems. Under stressmuscles tend to cramp. If we, during teaching Motility, are relying on a precise and repeated practicing of a border-controlled muscle action with an adequate carry-out (frequency and flux of the movement) the therapeutic effects on the muscle-nerv-action will in the end have the target direction on the Tonicity, the tone of the movement, the underlying power. We see in it a mental process which is neatly coupled to practicing with the carry-out of a strictly controlled movement during the treatment which is going to involve the next effect namely the Coordination of agonists and antagonists during the action. Here it is quite essential the movements to be carried out very consciously. We, of course, would not ask the patient that he should, precisely from the moment on when we start teaching him the correct movement sequences as for example deglutition for now and ever would have to carry out this movement under a fully conscious control. Just think of the state of the respective system during the sleep phase! Therefore it is our last but not least task to anchor the movement scheme with the full list of counted up qualities into his subconscious. In my opinion the most difficult part of the game. Under this point of view we might state that in the follow-up of the Qualities as we have lined them up always the next one promises a next higher degree of difficulty. This is the reason why I do not use the "from the gut" method. For me difficulties become more manageable if they are brought under strict control - through a sufficient planning of the procedure. In our metier planning first of all means : What is the purpose? We can not accept from the outset that all the Qualities of the Physiological Frame are deranged. This is why we need a Screening Test to determine the extent of damage the, as we above stated, broken link of the chain. As mentioned at the beginning, the succession of the Qualities does not only fit to the Therapy Management it, as well, gives the chronology of the tests for the examination. And, as also repeatedly said, we do have so many Myofunctional Exercises at hand that would not be so hard to find an appropriate one for each Quality to be tested what made me develop a method and scheme with the "Diagnostic Exercises" which you will find on this website under the link [DIAGNOSTIC EXERCISES/myonet].
If you have worked yourself and the patient through all the 29 test exercises your notes we draw quite clear a picture of the state of the system examined and where it bears it weak spots. That, again, gives reliable hints to how the therapy planning should have to look like. This again takes me back to my remark that it does not appeal to me to use some method from a famous Doc XY. If you approach an orofacial problem in the described way a method will come about, your method, and the one especially tailored for that patient. The XY method is quite easy to be prescribed by a therapist because it offers simple all-round program delegating the responsibility to Doc XY. Sure it will never be. Sure is to tailor the therapy especially to the one patient, from an exercise collection - or from this website. The exercises on this site mainly derive from the book: Thiele,E.: Myofunktionelle Therapie, Katalog der Übungen zur neuromotorischen Funktionsregulation, Heidelberg 1997, ISBN 383040185X, Hüthig Buch Verlag, Band 3. What you have in front of you is an in detailed revised edition which is in large part illustrated. By and by I hope to make these pictures appear as animations (as they already are present in the Diagnostic or the Tonometer Exercises). This will have the great advantage: You as the therapist might not be able to demonstrate it always in quite the same correct manner and without moving some neighbouring muscles. This is what the sketches can relief you from. More over children love screen pictures. And for the individual therapy the therapist will just copy the pictures accumulated on one file and burn it on a CD to hand it out to the patient for practicing at home. |
continue with "Survey" :

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}