exercise
,DRAWER-IN'-EXERCISE
Myofunktional Exercise Collection
|
Start |
Contents |
MFT-Start |
to the Catalogue |
MFT-guide |
MFT |
Catalogue |
|
|
028 exercise |
,DRAWER-IN'-EXERCISE |
Myofunktional Exercise Collection |
|
Application: |
to enlarge click picture |
|
This exercise is suitable for a (tendency of) proversion of the mandible. It is used with stomatognathic syndromal disorders and dysfunctions to gain an adjustment of posture and relief for the temporomanibular joints and pterygoid muscles. For orofacial problems the habituating of a physiologic posture through this exercise leads to an Eutonization of the immediate surrounding muscular areas. Therefore the patient should be able to take up this position before starting the actual and disorder specific therapy respectively the exercise being integrated into the initial phase. There is a special indication with nibbling or gnawing at things ( see Discussion). In the craniocervical respect there should develop a dorsoventral balance being of great significance for a free passage of nerve and blood paths. ,DRAWER-IN’ is part of the BASIC-POSITION. |
|
|
Contents: |
|
|
This exercise offers the training for a continuous self control and generates the feeling of a eutonized and well balanced posture of the mandible as its regular position as well as its starting position for MFT-exercises within the physiologic standby tone. It equally serves the patient for a reorientation when getting aware of parafunctions. Habituation in combination with Mental Training before falling into sleep ( in combination with TEETHCLICKING). |
|
|
Materials: |
|
|
Not required. |
|
|
Procedure: |
|
|
- Previous exercises: Should be the SITTING-POSITION during therapy sessions. In complicated cases orientation should be sensed and controlled by the patient with the exercise THE PEA. |
|
|
-Starting position: ,DRAWER-IN’ |
|
|
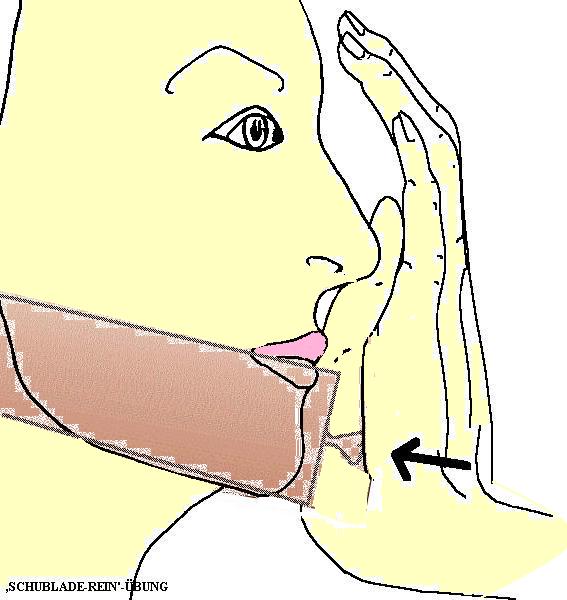
- Step-by-step-description: -1 The patient takes up the bite-off-position where the incisal edges of the front teeth are positioned upon each other. -2 The flat of the therapists hand – later on of the patient – is positioned on the face in a way that the carpus area of the hand is lies on the chin tip (like head-in-hands). -3 While the hand now exerts a light pressure the mandible immediately gives way straight backwards till the “end”. |
|
-Timing : During the sessions the position is kept while counting to twenty followed by a relax pause followed by a repetition about five times. In the beginning this prescription should be transferred to the domestic training. Later on the posture will be taken up consciously and monitored frequently during the day as well as when preparing to sleep. With the therapy progressing this exercise will be replaced by the ,M’-POSITION. |
|
Characteristics: |
|
Stereognosis, habituation, (Information), orientation, myobalance, resting position, coordination, static, tone, (manipulation during the start phase). |
|
Remarks: |
|
With the mentioned difficult cases of a protruded mandible position the finger-tip control - feeling the joint head – in the preauricular region (THE PEA) should be prescribed at least during the starting phase. With a tendency for grinding or pressing the keeping of the mandibular resting position should be observed (TEETCLICKING / Mental training). |
|
Discussion: |
|
,DRAWER-IN’ is part and propaedeutic exercise for the RESTING POSITION and by this equally of the BASIC POSITION (see there) and so will be taken up in connection with Mental Training before sleep (here especially indicated with bruxism and the like as well as sleep apnoe , snoring.) This is recommendable as hyperactivity, hypertone, dysfunction and spasms may not be restricted to our border lines of the schematically predetermined muscular regions of the system. Therefore mainly the Basic Position should be muscularly balanced spaciously especially and well-directedly for the pterygoid musculature. With an existing suspicion on the gnathologic sector that the disc of the temporomandibular joint might show tendencies of moving prematurely ahead of the joint head it should be affirmed that the adductor muscles do not exhibit hypertone. Regarding the anatomy of a hanging joint we should assume a fatal synergism of adductors and pterygoids using the discus as a battering ram and thus pushing it or squeezing it forward in front of the joint head. (Not rarely the gliding motion of the joint head in relation to the disc is progressing asynchronously and incoordinate.) In that case we should employ the TAP-TAP and the manipulated JOINTSTRETCH as simultaneous exercises. With the before mentioned indications of nibbling or gnawing we find malfunctions like lip or beard nibbling ( the latter only with elderly masculine patients) where the patient shoves the mandible forward to grasp material with the edges of the incisors. Certainly most patients do not realize that in the physiologic jaw position the incisal edges of the upper front teeth do overlap those of the lower ones in the occlusion with about 2 mm . These patients “suffer from an overbite” as they themselves do describe it and therefore push the mandible forward in a misunderstood self-correction as often as possible to improve their appearance. We find this also with media obsessed (extroverted) people talking ( in front of a camera). In those cases usually an instruction may be sufficient as the therapy method of choice. Many habits in our field develop symptoms that can be found described with disorders of a similar genesis in the whole body as the Multiple-Movement-Syndrome. |
|
Instructions: |
|
The chin must not be protruded like the bumper of a car or stay open like a forgotten cupboard drawer which tends to hit ones shins. Just imagine that someone is pressing the flat hand against your face from the front pushing the drawer (the chin with the lower jaw) inwards. Of course you may do that yourself. Put your flat hand upright on your face and slightly press against your chin. The chin will put up resistance. The lips are rested upon each other as when you articulate an ‘M’. now move your jaw slightly up and down while the chin does not press against your palm but stays back. If this works out all right the drawer will be allowed to move forward – and immediately the palm shoves it back again. Then the chin may be moved faintly up and down but stay in the rear position. This should be repeated 10 times. Stay relaxed! |