general chapter
JOINT-EXERCISES
Myofunktional Exercise Collect ion
|
Start |
Contents |
MFT-Start |
to the Catalogue |
MFT-guide |
MFT |
Catalogue |
|
|
201 general chapter |
JOINT-EXERCISES |
Myofunktional Exercise Collect ion |
|
Application: |
to enlarge click picture |
|
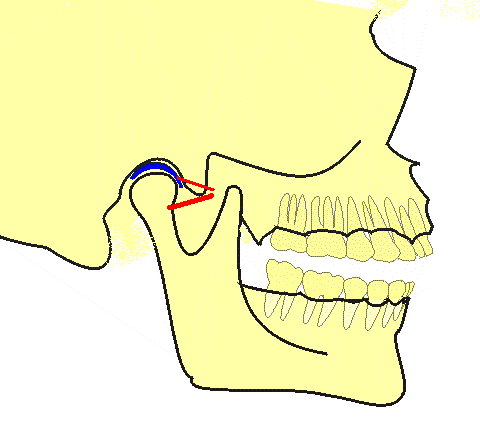
This chapter gives a general description of a collective group of exercises and details which are sharing the here described facts. Joint exercises for the TMJ (Temporomandibular Joints) are used in cases where the joints are affected or already show symptoms of pathological alterations such as joint noises or aching or alterations in the physiological movability. Among the dysfunctions are the static ones at one hand, as jaw pressing or a protruded posture, at the other hand the kinetic ones as the non-physiologically wide or frequent protrusion or laterotrusion (excursive movements). |
|
|
Contents: |
|
|
The contents of the joint exercises are exercise specific and, thus, described more in particular in the respective chapters. Generally they answer the purpose of realisation of the problems, acquiring of a physiological frame of movement and the loosening of spasms in the musculature, (Anatomy 1.6, Area VII, Page 31). |
|
|
Materials: |
|
|
Exercise specific. |
|
|
Procedure: Exercise specific. |
|
Characteristics: |
|
The character of the exercises is quite different; generalizing it may be stated that they commonly show sensitising and orientation in their contents. |
|
Remarks: |
|
To guarantee a physiological joint function it needs an intact system. This (Stomatognathic) system integrates Maxilla and Mandibula with the osseous jaw arches and intact dental arches which will have to intercuspidate in a well defined manner (occlusion) as to manoeuvre the actions of the masticatory muscles and, in a wider sense, those of the orofacial an neck muscles via a sensitive feedback system together with the control centre in a way that lastly the triggering of dysfunctions will be omitted. Much importance is attached to the occlusion (static and dynamic). If the dentition might have been already badly affected the cooperation with a gnathologist is warmly recommendable and perhaps a splinting with a function splint as an interim solution. |
|
Discussion: |
|
As suggested above with the respective problems the diligent checking and, if needed, correction of the intercuspidation should be carried out. The exercises listed up below may render useful assistance in Therapy or are in fact essential to cancel entrenched dysfunctions. They include most different contents and are partially located rather in the physiotherapeutic range. Some will have to be carried out with the aid of an assistant person (or by the therapist); partially they may be learned and habituated by the patient. Basically the entire orofacial musculature should be checked and subjected simultaneously to therapy. In this connection a correct tongue positioning and function as well as lip closure and cheek tonicity play an important role. (In this context see also Anatomy Page 10 illustration and text). The exercises for these areas are not included in the below listing. |
|
Instructions: |
|
(Arranged in alphabetical order) On this see the single descriptions of the respective exercise chapters. |
List of Exercises
OPEN AND CLOSE
Controlling the Adductor employment.
BALLOON
Important for he cheek tonicity with cheek pressing or biting.
CHUBBY LIP
Preventing of Mentalis pressing, lower lip biting (Front teeth arch deformation).
THE PEA
Acquiring the retral position of the TMJ condyle.
PODGY TONGUE- SLIM TONGUE
Correction of the tongue tonicity in a lateral tongue pressing or biting-on.
JOINT STRETCH (MANIPULATED)
Physiotherapeutic, demonstration of a joint easing and muscle loosening.
BASIC-POSITION
General posture of the upper body.
COLLUM EXERCISES
These exercises should be considered as attendant methods for the Collum musculature.
NECK SIDE STRETCH "
POSITION EXERCISES "
JIG-EXERCISE
Self manipulated support for the retrusion of the mandible.
MASTICATORY MUSCLE
Manipulated stretching of mainly the Musculi Pterygoidei.
ROLLING HEADS
TURN YOUR HEAD
EASY NODDING
Physiotherapeutic backing measure for the Collum Vertebrae.
CLOWNY
Lip closure as a potential trigger problem.
,L-M’-POSITION
Obligatory stand-by posture for the Orofacial System.
,M’-POSITION
Obligatory stand-by posture for the Stomatognathic System also called the Physiological Rest Position.
MASSETER EXERCISE
Checking the tonicity of the Adductor musculature.
GAPE
Self manipulated mastication muscle stretching.
MENTAL TRAINING
Important basic condition for a nocturnal self monitoring.
, M-O-I ‘
Adjustment for the “Aged Face” (accompanying symptoms the “derailed features”).
TIRE OUT CHEWING
Presumably mental exercise to correct Adductor hyperactivity.
NAPE-DIALTOR
These exercises should be considered as
attendant methods for the
Collum musculature.
PLATELET-HOLDER
Attendant method for the mouth slit closure.
DRAW-BACK
Attendant method for the tongue retroversion and slim posture.
RESTPOSITION
Especially for the night time habituation of the correct Mandibula position.
TUBECHEWER
Adductor relaxation.
HOSECLAMP
Adductor relaxation.
,DRAWER-IN’-EXERCISE (CHIN-IN)
Acquiring the basic principle of the jaw positioning.
SLENDER TONGUE
Attendant method for the tongue retroversion and slim posture.
SIDE THRUST
Self manipulation stretching of the Pterygoidei.
SITTING-POSITION
Common attendant measure body posture.
,TAP-TAP’-EXERCISE
Acquiring the self manipulation for an Adductor relaxation.
CHEEKBUMP
Attendant method for cheek pressing.
CHATTERING TEETH
Autogenous Adductor relaxation.
TEETHCLICKING
Night time mental monitoring for Adductor hyperactivities.