exercise
MASSETER EXERCISE
Myofunktional Exercise Collect ion
|
Start |
Contents |
MFT-Start |
to the Catalogue |
MFT-guide |
MFT |
Catalogue |
|
|
118 exercise |
MASSETER EXERCISE |
Myofunktional Exercise Collect ion |
|
Application: |
to enlarge click picture |
|
Main area is the OHM (Open Mouth Habit) but, as well, the so called chewing sluggishness and the tendency for a hanging mandibula (see also notes in the paragraph “Discussion”). The target area besides the one addressed in the specification (: VII/1, Page 31), is the whole adductor musculature (Area: VII, Page 31). |
|
|
Contents: |
|
|
Strengthening and hold exercise under an excessive tonicity in biting together in the centric occlusion. |
|
|
Materials: |
|
|
Not obligatory, see paragraph “Discussion”. |
|
|
Procedure: |
|
|
- Previous exercises: Are especially the adductors aimed at to be uprated no particular pre-exercise is needed. In case of the Habitual Mouthbreathing see chapter MOUTHBREATHING. |
|
|
-Starting position: No prescriptions; a coordinated pre-tensioning (Standby-tonicity) through taking up the Standby-position (see also RESTPOSITION, ,L-M’-POSITION is advisable. Worth respecting is the retroversion of the Mandibula and this throughout the whole work-out (,DRAWER-IN’-EXERCISE (CHIN-IN)) |
|
|
- Step-by-step-description: -1 The first and likewise most important step of this exercise procedure is the thorough instruction of the patient about the importance of a guarded “standard position” (see RESTPOSITION), the demonstration of the Masseter muscle belly (myogaster) during the adductor straining, furthermore the habitual intercuspidation position and the joint posture (PEA). -2 The (molar) teeth are set upon each other, initially under control of the correct position through the therapist (see “Discussion”). -3 The tonicity in the occlusion will, now, be increased, at first ( or throughout the practicing) with a palpating control through the finger tips bilaterally on the Masseter belly forming with the action just above the Mandibular Angle without letting arise discomfort with among the teeth (see notes). This position is pertained while counting over a shorter period. Consequently the start position is regained. |
|
-Timing: In form of a hold-exercise the round makes one sequence the extent of which should not be measured to lengthy; it should be counted to ten, roughly. This solely stato-dynamic exercise may easily be combined with the kinetic OPEN AND CLOSE in form of an ALTERNATIVE EXERCISE to make one series. |
|
Characteristics: |
|
Hold exercise, tone rising, Sensitivity (sensory feed-back), organ stereognosis, Motivation. |
|
Remarks: |
|
With the mentioned ‘chewing sluggishness’ or the OMP (habitual open mouth position) it should be thoroughly tested if the adductors (pars pro toto “Masseter”) in fact show an incompetent tonicity; a differential diagnosis would be the appearance of discomfort within the joints or single periodonts in jaw occlusion – here the exercise would be contraindicated. The mentioned testing might be done with a clothes peg. This exercise should not be the cause of nurturing the patient to bruxism. |
|
Discussion: |
|
As many patients tend to position the incisal edges of their front teeth upon each other in an end-to-end bite with the request to ‘bite together’ there should be given precise instructions about that. Likewise it should be seen to the molar teeth of both sides getting in a level contact, the mandible neither being shifted for- nor backwards neither unilaterally (Laterotrusion). In this connection it should be checked whether the dentition permits a successful practicing of this exercise. If considerable disorders in the static occluding interlocking (frequently with a ‘mixed dentition’) would be notable an even and powerful biting together will not be producible and thus the exercise not be verified. The merit of this exercise presumably lies in the Motivation as the patient will easily be able to follow the ongoing action by palpating the Masseter belly in self evaluation (sensory feedback). As already mentioned before, in this field much more frequently dysfunctions are spotted due to hypertone or hyperactivity. This is why before a prescription of the discussed strengthening exercise at least all symptoms should be reviewed in the aspect of the chewing functions being complied and moreover whether true ‘Hypo-Symptoms’ are to be established (Hypo-: Sensitivity, Tonicity, Mobility, Motility). For this purpose an exercise variation can be chosen in which single-sided in a change a wooden clothespeg is set between the molar teeth to be opened and shut slowly. From the number of executed repetitions a conclusion may be drawn about the real physiological capacity of the musculature. A further benefit of this variation of the MASSETER EXERCISE is the fact that in a fluent motion process an isokinetic straining is required. Following the postulation to design MFT-Exercises as functional as possible the latter method would rather match the chewing procedure and, thus, avoid the danger of inducing a dysfunction. A quite similar result however with a lesser training efficiency is gained wit a variation where the patient is chewing on rubberlike objects. On this matter see also TUBECHEWER outlined in the paragraph “Discussion” of the chapter TIRE OUT CHEWING, HOSECLAMP among the MOTIVATION EXERCISES or the method where the patient is chewing on half-centimeter sized rubber chinks (danger of swallowing). This exercise resembles still more the physiological action. In all cases of chewing on resilient materials (rubber) there will be missing the pressure absorption resulting in the decay of the material which may give rise to a nonphysiological straining and thus damaging of the periodontal tissues and furthermore this will alter the course of the single motion. The variation of chewing on gum will match this postulate most likely but is still less controllable in its carry-out and is bearing the risk of an induced Hypermotility (or at least Hyperactivity). It would be the optimal way to get an influence upon the eating habits of the patient , for example, to consume more coarse food making a more intensive chewing necessary and generally to ensure that the chewing process will find greater attention. Muscle weakness (Hypotonia) is indeed rather not so frequently the cause for an open moth posture. Much more often this muscle area is afflicted with hyperactivity with a multitude of unfavourable and noxious symptoms. Therefore it should be avoided with the utmost precaution to bring the patient in such a situation or to increase the disorder in case of its presence. So it should be ensured the prevailing debit to comply with the functioning frame being in fact attributable to adductor hypotonicity. For the mouth and jaw posture not only the adductors are responsible but in a broader sense also the airways respectively a freely passable nose breathing, the tissue and muscle specific practicable lip closure (Orbicularis insufficiency or Hypotonicity), The tone of the cheeks, the tongue posture in rest and action (interpositioning ) and the physiological hypobaric pressure in the Cavum Oris, again, being subordinate to the Velum and Pharynx musculature respectively the state of the textures in these areas (about this also see remarks in the chapters TONGUE PROP, REAR ORAL CAVITY, and MANDIBLE EXERCISES. |
|
Instructions: |
|
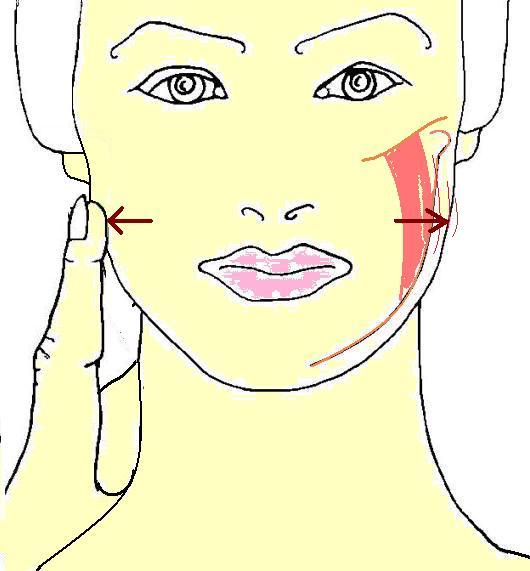
We will, now, settle on fixing the Masseter, the chewing muscle running from the ear down to the jaw angle back at the cheek. When strained it develops a bulky belly like a strong arm muscle. It shows a bulge which you can feel on both sides near the bony angle. At first the molar teeth are positioned on both sides evenly upon each other. Then the finger tips are positioned on the described spot in front of the ears. If you, now, bite the teeth together the muscle belly will become clearly palpable. Slowly count to ten while keeping the tension evenly. Then get a break and afterwards the repetitions as often as we agreed upon. By the way, your teeth should only be bit on in this exercise! Otherwise they should always be in the ,L-M’-POSITION. |